
Serving Midwest Aviation Since 1960
Serving Midwest Aviation Since 1960
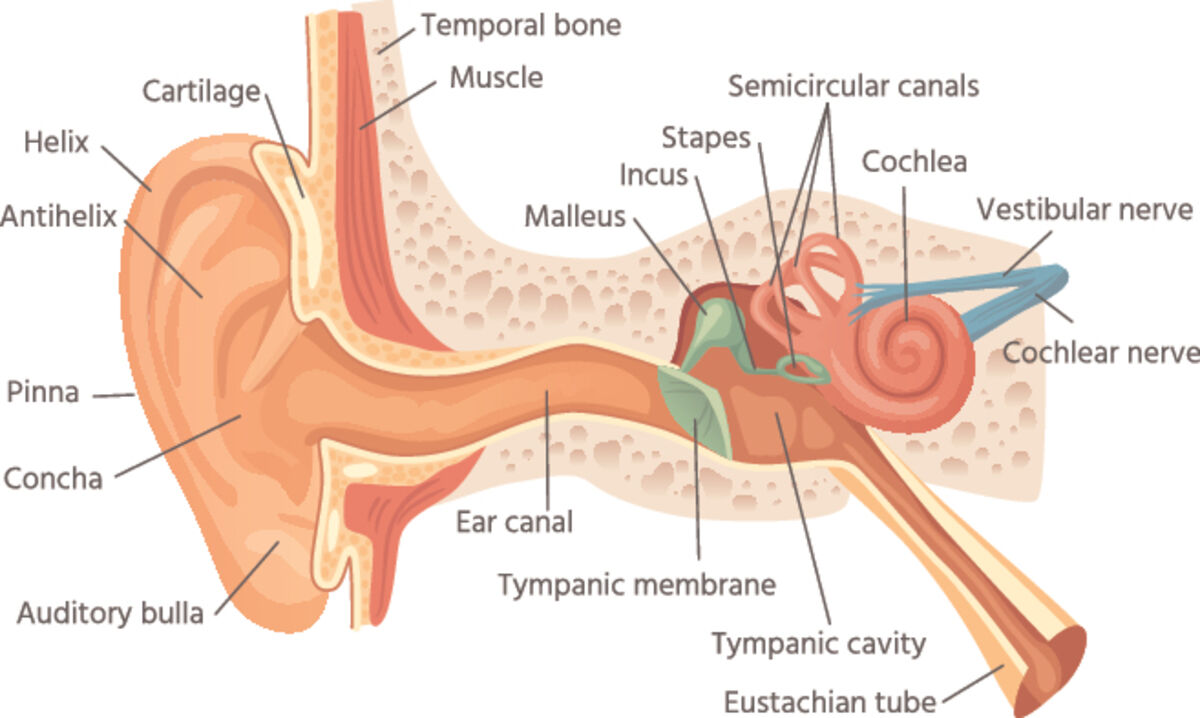
The body's "vestibular apparatus" is located in each inner ear.
Vertigo is a common experience. It's not just a feeling of light headedness but a sensation that the world is spinning around. When you were a kid and spun around you intentionally set off a form of positional vertigo. Something like that can happen in flight. For example, when you're in the clag and abruptly bend down, let's say to pick up a pencil; suddenly it seems as if either you or the plane is in a spin.
Hold still. Don't do anything funny with the stick and it goes away. Accelerate rapidly and the aircraft seems to be pitching up. Slow down quickly and it seems to pitch down. In all of...

Reader Comments(0)